Western Veterinary Specialist & Emergency Centre

What can we dig up for you?
What can we dig up for you?

Western Veterinary Specialist & Emergency Centre
Western Veterinary Specialist & Emergency Centre
403-770-1340
Spitfire
1.5-year-old female intact Domestic Short Hair
Spitfire presented to the emergency service at Western Veterinary Specialists and Emergency Centre after an unwitnessed fall from a 7th story balcony. The owners suspect that she fell onto a car and she was then discovered under a vehicle.
On her initial physical exam, her vital parameters were within normal limits. She had a small laceration on the left calcaneus and she had scleral hemorrhage in the left eye. Her neurologic exam identified that she was paraplegic with intact nociception in both pelvic limbs and tail. Her perineal reflexes were intact. Her patellar and withdrawal reflexes were decreased bilaterally. The remainder of the neurologic exam was unremarkable. Based on neurological exam findings a lesion localizing to L4-caudal spinal segments was determined. Primary differential diagnoses for this lesion included a spinal fracture/luxation vs. a traumatic disk extrusion.
A complete blood count, serum biochemistry and full body radiographs were performed. The blood work was consistent with acute inflammatory changes as well as an elevated ALT. This is likely due to muscle trauma and/or hepatic damage associated with the fall.
On survey spinal radiographs there was a comminuted transverse fracture of the spinous process, body and arch of L5 with minimal displacement. The L4-5 intervertebral disk space was narrowed as compared to adjacent sites. The caudal endplate of L4 is also fractured. (Figure 1a and 1b)
 Figure 1a
Figure 1a
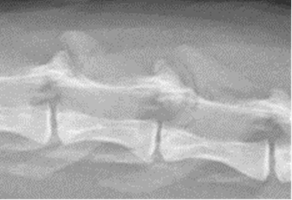 Figure 1b
Figure 1b
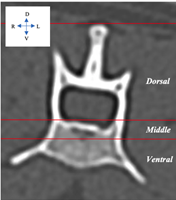
Vertebral fracture and luxations are considered with respect to the three-compartment model of the spine. This model considers the dorsal, middle and ventral compartments of the spine to estimate spinal stability. The dorsal compartment includes the supraspinous ligament, interspinous ligaments, ligamentum flavum, spinous processes, articular processes, laminae and pedicles. The middle compartment includes the dorsal longitudinal ligament, dorsal annulus and the dorsal vertebral body. Finally, the ventral compartment included the remainder of the disk (annulus fibrosus and nucleus pulposus), vertebral body, and the ventral longitudinal ligament. It is important to understand which portions of the spine are included in each of the compartments, because if two or more compartments are affected, then spinal stabilisation is typically advised. (Figure 2)
Aside from the three-compartment model of the vertebral column, surgery is also considered for patients with severe neurologic deficits and pain. There are a multitude of ways in which vertebral column fractures can be stabilized. Most commonly, this is accomplished with positive profile threaded pins and bone cement (polymethylmethacrylate - PMMA). Other options would include bone plates, screws and PMMA and external fixators. Medical management of vertebral column fractures may be considered for patients whose fractures are considered stable (ie; less than 2 compartments involved), with no to minimal neurologic deficits and who can be managed effectively on oral pain medications.
Prognosis is determined similarly to patients with intervertebral disk extrusion and is dependent on the findings of the neurologic exam. In patients who have no motor function in the pelvic limbs, it is necessary to test for deep pain sensation (nociception). This is different from the withdrawal reflex and requires a behavioural/physiologic response to having their digit pinched to be considered positive. Behavioural/physiological responses may include trying to bite, looking at the pinched toe, crying out etc.
If they are deep pain positive, there is about an 85% chance that the patient will recover to normal function after surgery. This means we anticipate that they will be able to walk, urinate and defecate normally, as well as live a pain free life. Some residual neurologic deficits may persist. If there is no deep pain, there is a less than 5% chance of the patient walking or maintaining continence. Thus, in cases of deep pain negative spinal fracture/luxation these patients are generally euthanized. It is crucial and important to note these statistics are different from cases of simple intervertebral disk extrusions which generally have a better prognosis; 95% chance of recovery if deep pain remains intact and 50-60% chance of recovery if they are deep pain negative.
Complete assessment of vertebral trauma in dogs currently requires CT and MRI for evaluation of the osseous and soft tissue structures that contribute to vertebral stability. A CT is considered gold standard for spinal fractures as it is reported to be the most sensitive and specific imaging modality to identify and classify the morphology of the osseous vertebral trauma. A major limitation of CT is its ability to assess the parenchyma of the spinal cord and it should be mentioned that MRI is considered the best imaging modality to assess soft tissues, image the extradural, intradural and spinal cord compartments. In clinical cases, due to availability and financial reasons, we often have to make a choice as to which imaging modality is going to be most valuable. For suspected fractures, a spinal CT will most often be performed to document fracture morphology and aid in surgical planning.
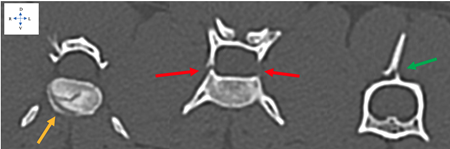
In Spitfire’s case, the CT scan identified fractures of the right transverse process at L2, L3 and L5. More importantly a short oblique fracture of the caudal endplate of L4 was seen. Additionally, fractures of the L4-5 facet, the right and left pedicles of L5, and the L5 body and spinous process were noted. Based on CT images, minimal extradural compression of the spinal cord was noted indicating that the most significant portion of her injury was the fracture itself rather than a traumatic disk extrusion. As previously discussed, an MRI of the lumbar spine would be required to fully investigate the relative contribution of a traumatic disk extrusion and the degree of spinal cord swelling. (Figure 3)
Spitfire was taken to surgery immediately following the CT scan based on instability of the identified spinal fractures (all three compartments affected) and her severe neurologic deficits. The right and left sides of the vertebral column were approached and the L4-5 vertebra were identified. Gross instability was evident at this site. As the fracture was not displaced, reduction was not necessary. One positive profile pin (2.0 mm in diameter) was placed on both the right and left sides of the L4 vertebra. Two pins were also placed into the L6 vertebra, spanning the fractures of the caudal L4 and L5 vertebra. The pins were bent towards each other and the construct was then stabilized by encasing these pins in bone cement. A post-operative CT of the lumbar vertebral column was then performed to ensure the pins were appropriately positioned. The surgical aim is to orient the pins at an angle of 30-60 degrees from the sagittal plane in order to avoid the trauma to the spinal cord and the aorta (Figure 4). Same day, post-operative lumbar spinal radiographs were performed to monitor and trend fracture healing at the 8-week re-check appointment. The surgical repair was deemed acceptable; however, upon evaluation of post-operative CT and radiographic images, the ideal pin depth in the vertebral bodies would be 2 mm shorter (Figure 5). No attempts for surgical revision were made as the risks did not outweigh the benefits of altering pin position.
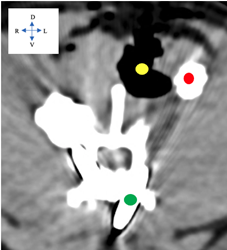
Figure 4: Post-operative CT scan at the level L4. Soft tissue window with metal suppression algorithm applied to minimize metal streaking artifact. Note the subcutaneous emphysema (yellow) associated with the surgical approach. Red represents the cranial extend of the PMMA. The metal pins (green) in the pedicle and body of the vertebrae. The safe window between spinal cord and aorta in this patient was <1 cm.

Figure 5: Post-operative spinal radiographs. Note the pins in the L4 and L6 vertebra. The pins have been bent towards each other and encased in PMMA to stabilize the vertebral fracture.
Spitfire was paraplegic with intact nociception on her initial neurologic exam. The day following surgery she was mildly improved and considered to be non-ambulatory paraparetic, with stronger motor function on the right pelvic limb. Her reflexes remained decreased. She was discharged to the care of her owners on day 3 post operatively. Two weeks after surgery she was nearly ambulatory and paraparetic (right still better than left) and her spinal reflexes were normal. Her ALT had improved to normal. Given her rapid improvement, she is expected to have a complete recovery. At Spitfire’s 8-week post-operative re-check appointment, in additional to a full physical and neurological exam, repeat lumbar spinal radiographs will be performed to evaluate fracture healing and ensure integrity of the surgical repair. If all is well at that time, she will be allowed to return to normal activity levels.
Please enjoy reading about one of our Cardiology Patients Dexter.
Dexter 6-month-old male intact Miniature Dachshund
Dexter presented to our cardiology service for evaluation of a continuous heart murmur, incidentally noted by his referring veterinarian during his vaccine appointment. On initial physical examination, a grade 5/6 left axillary continuous murmur was ausculted, often described as a “washing machine” murmur due to its characteristic sound. An echocardiogram was performed, which confirmed a left-to-right shunting patent ductus arteriosus (PDA), with mild left ventricular enlargement, mild to moderate systolic dysfunction, and mild left atrial enlargement.
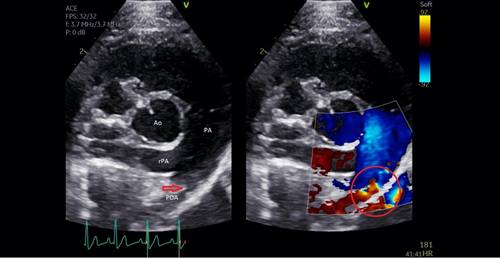
Figure 1 PDA visualized on echocardiogram (left). Colour Doppler on right shows blood flow across PDA site.
The ductus arteriosus allows shunting of blood across the pulmonary artery to the aorta during fetal development, bypassing pulmonary circulation and preventing volume overload in developing lungs. Following birth, lung inflation and stimulation of the pulmonary circulation occurs. The increased blood flow into the pulmonary veins results in increasing left atrial pressures, which stimulates ductus closure. The ductus arteriosus usually closes within 24 hours of birth, preventing deoxygenated blood in the pulmonary trunk from entering the aorta. In patients with a PDA, the ductus arteriosus fails to close. The etiology is not fully understood in animals; however, is it hypothesized that hypoplasia of the smooth muscle of the ductus results in a failure of contraction.
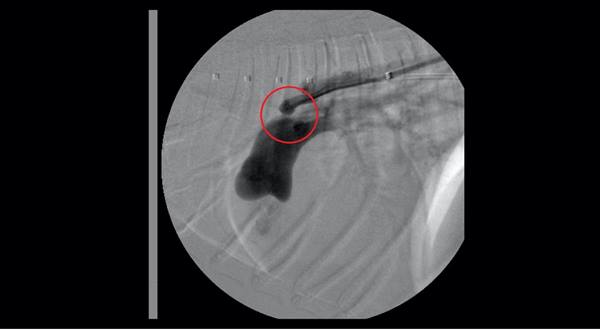
Figure 2 Angiography of the PDA site, with contrast shunting from the aorta into the main pulmonary artery.
Left untreated, the left-to-right shunting results in systolic dysfunction, volume overload, arrhythmias, and congestive heart failure (65% within first year of age if uncorrected). Other complications include development of severe pulmonary hypertension resulting in reverse shunting (right-to-left), exercise intolerance, and cyanosis. A left-to-right PDA can be surgically ligated or corrected by minimally invasive device occlusion using an ACDO device (Amplatz® canine ductal occluder). The ACDO device is self-expanding nitinol wire mesh, with a flat disk to secure the device and an expanding waist to occlude the PDA. Success rates are similar for the procedures (94 vs 92% respectively), however lower complication rates are reported with minimally invasive techniques.
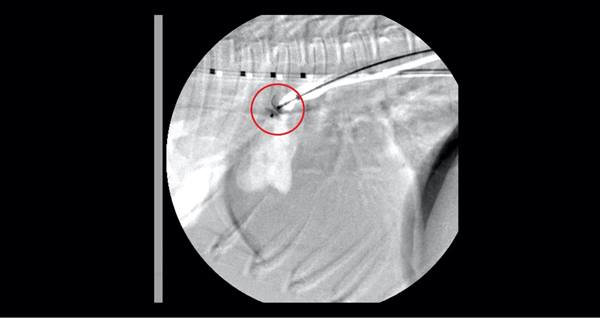
Figure 4 ACDO device being placed across the PDA site.
Dexter was taken to surgery for correction of his PDA, using a minimally invasive approach. An Introducer catheter was fed up the right femoral artery and into the aorta using fluoroscopic guidance. Angiography was performed to determine ductus size for placement of the occluding device. A guidewire was then fed across the PDA site into the pulmonary artery. The ACDO catheter sheath was fed across the PDA site, and the ACDO device was deployed using fluoroscopic visualization. The distal disc opens into the pulmonary artery, and further deployment of the device fills the PDA ostium with the waist of the occluder. The device placement was confirmed with fluoroscopy. The femoral artery was then ligated upon completion of the procedure.

Figure 3 ACDO device, actual size on left. Magnified on right
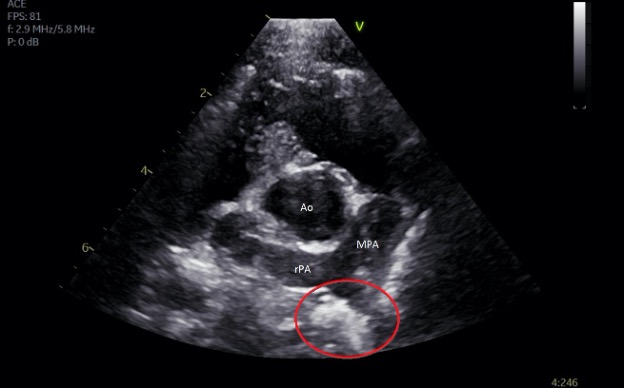
Figure 5 ACDO device circled in red. Image taken 12 hours post-occlusion.
Dexter’s ACDO device was visualized with echocardiogram the following morning, confirming no residual transductal flow. He was discharged to the care of his owners later that day and is now happily hiking mountains and enjoying being a puppy!

Lexi, 8.5-year-old female spayed Havanese
Lexi presented because of recurrent bladder stones. Two years ago Lexi had a cystotomy performed because of bladder stones. Upon stone analysis the stones returned as calcium oxalate. Lexi was placed on a prescription urinary management diet. In March 2021 the owners suspected that Lexi had a urinary tract infection and brought Lexi to see her family veterinarian. She was treated with antibiotics and improved, but she would occasionally have hematuria at the end of her urinary stream. Upon investigation, it was discovered Lexi had multiple bladder stones. She was referred for investigation of possible minimally invasive techniques for their removal.


Figure 1 Lexi’s abdominal radiographs from May 18th, 2021, showing multiple bladder stones, suspected to be calcium oxalates
Calcium oxalate (CaOx) stones in the lower urinary tract are quite frequent. They represent almost 50% of lower urinary tract stones in dogs, and older, small breed dogs are predisposed. Miniature schnauzers, Lhasa Apsos, Shih tzus, Yorkshire terriers, and Pomeranians represent some of the breeds that have a higher incidence. Males seem to have a 1.5-2 times greater risk of developing these stones. Even after removal and preventative treatments, there can be a 50% recurrence of these stones.
Their formation is a complex interaction of multiple factors: from diet to breed predisposition, to a disequilibrium between promoters and inhibitors of calcium oxalate crystal formation. Because of these complexities, prevention is quite difficult and frustrating. Screening and management of predisposing factors is important (ex: hyperadrenocorticism, hypercalcemia disorders, dietary and medication factors, obesity), but often this is not enough to prevent these stones.
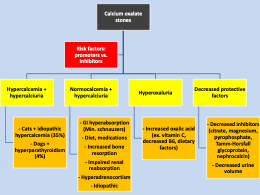 Figure 2 The formation of calcium oxalate stones in the lower urinary tract is due to complex interactions of multiple factors
Figure 2 The formation of calcium oxalate stones in the lower urinary tract is due to complex interactions of multiple factors
Diagnosis is relatively straightforward as once formed these stones are very radio opaque. Urinalysis may or may not indicate calcium oxalate crystalluria (not always present) when stones are formed, but the presence of CaOx crystals in predisposed breeds should prompt cause for concern. There is some evidence that predisposed breeds should be screened regularly for CaOx crystals and stones at the age of 7-8 years of age through urinalysis and abdominal radiographs. Urinary calcium-to-creatinine ratio has also been shown to help screen which dogs will be more predisposed to forming these stones.
Once CaOx stone present, removal via traditional surgery (cystotomy) has traditionally been the treatment of choice. First-line prevention is often aimed at changing a dog’s primary diet to a prescription urinary diet management and increasing water intake. Despite this, many dogs will have reoccurrence and the prospect of another cystotomy can be difficult to accept.
Surgery is reliable and predictable. However, minimally invasive procedures to remove these stones do exist but are not applicable in all instances. It is important to know their limitations and when to apply them. In general, it is best to detect stones when there are few of them for these procedures to be successful. For dogs who have had CaOx removed, we recommend screening them every 3-6 months depending on the dog for recurrence, because detecting earlier stone formation (ex. 1-2 stones) will make it much easier for these stones to be removed).
Percutaneous cystolithotomy (PCCL) is a procedure whereby under general anesthesia a small 1-2cm incision is made into the abdomen to grab the bladder, and then insert a special port into its lumen. This port is then used to either perform cystoscopically-guided basket retrieval of stones or laser lithotripsy to break up the stones to then grab them with a basket. PCCL is as effective as traditional cystotomy with fewer complications and a shorter recovery time.
Laser lithotripsy is where bladder stones are fragmented using a holmium, and then the fragments are removed by cystoscopically-guided basket retrieval. However, there are several limitations to laser lithotripsy: its applications are only worthwhile when few bladder stones are present (usually 2-4 stones) due to the possible trauma caused by multiple cystoscopy entrances into the urethra as well as the longer anesthesia time if more stones are present, and also due to size and sex of dog (with male dogs, PCCL is often preferred as the flexible cystoscope has lower resolution than the rigid scope used in females, and can only accommodate male dogs greater than 8-10kg).
Cystoscopically-guided basket retrieval of stones, combined with voiding urohydropropulsion is possible especially in female dogs with a low stone burden. This was the approach taken with Lexi with Drs. Serge Chalhoub (internal medicine specialist, Faculty of Veterinary Medicine, University of Calgary) and Germaine Hung (surgery specialists, WVSEC staff surgeon). Under general anesthesia, the stones were visualized using a rigid cystoscope. The bladder was then filled with saline and the scope removed. Lexi was held in an upright position and constant manual pressure was applied to her bladder while holding a bowl under her vulva. Multiple stones were removed this way, then the cystoscope re-inserted into her bladder. Some stones were moved using a basket. These two procedures were repeated several times and all stones were removed. Stones were sent to the Canadian Veterinary Urolith Centre in Guelph for analysis.
 Figure 3 Lexi basket retrieval of stones
Figure 3 Lexi basket retrieval of stones
Lexi recovered well and went home that same day with no surgery necessary! She returned for a recheck exam and urinalysis 2 weeks later and the owners stated she had been doing quite well.
 Figure 4 Lexi and Dr. Chalhoub
Figure 4 Lexi and Dr. Chalhoub
Since this is Lexi’s second reoccurrence, other preventative treatments were started. Lexi was continued on a preventative urinary management diet, and also started on Potassium citrate to help keep her urinary pH in an adequate range for the prevention of CaOx. She will be monitored every 3-6 months (urinalysis and abdominal radiographs) for the deteetcion of crystals and stones. If stones are present then minimally invasive techniques will have a higher success of removing them and avoiding cystotomy. Thiazide diuretics can also be used to prevent CaOx formation. Therefore, for many dogs the management of CaOx stones is about maximizing preventative measure but also screening them to catch stone formation early to remove them in a minimally invasive way.
If your hospital would like more information on our referral services, please contact our referral coordinator today!


© Copyright VCA Canada Hospitals all rights reserved.
Affiliate of Mars Inc. 2024



